Blog: Thinking Outside the Box: Utilizing Eye Tracking to Diagnose Cervical Dysfunction After Whiplash
Acute head injuries can cause a cascade of pathophysiolgical processes and fluctuations of neurometabolites in the brain. Our goal is to pinpoint the complex pathology into concrete clinical diagnoses in order to provide the appropriate treatment paradigms. Diagnoses are not always straightforward, and we are still discovering the interconnectedness of the brain within itself as well as with other parts of the body.
An often overlooked aspect of head injuries are the concomitant neck injuries, most commonly whiplash associated disorders. Pain and inflammation caused by traumatic neck injuries can alter proprioceptive control of the cervical spine. These altered cervical afferents can directly affect ocular-motor functioning. This can be confusing or seem far-fetched, but I recently had a patent who was a textbook example of this:
Case Study
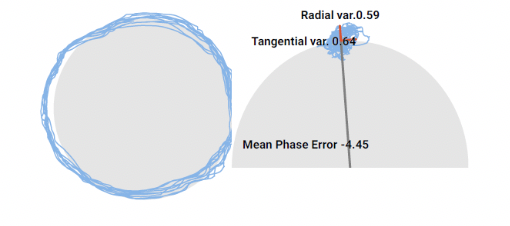
A 22 year old Division I athlete initially presented to physical therapy 2 days after high-speed motor vehicle accident. She was cleared of all cervical boney or ligamentous abnormalities via XRay and clinical examination. Initial symptoms included headaches, cranial pressure, fatigue, neck pain, and difficulty with concentrating, reading, and computer work. Diagnosis: cervicogenic dizziness and concomitant concussion with vestibular dysfunction. Cervicogenic dysfunction was diagnosed via clinical examination (limited range of motion, cervical musculature tenderness and hypertonicity, and positive cervicogenic dizziness testing) and further objectified by smooth pursuit eye movement abnormalities. Eye tracking was testing in a neutral neck position and then re-tested in relative cervical rotation consistent with the Smooth Pursuit Neck Torsion test. Interestingly, poor eye tracking (as well as subjective report of blurry vision) was only observed in relative cervical rotation (see B and C below).
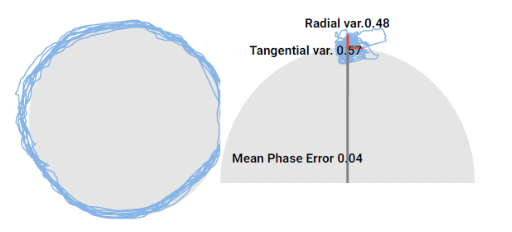 . A. Eye tracking in neutral neck position 2 days after car accident.
. A. Eye tracking in neutral neck position 2 days after car accident.
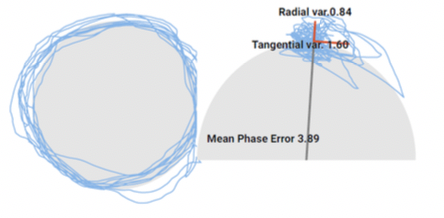
B. Eye tracking in relative right neck rotation 2 days after car accident.
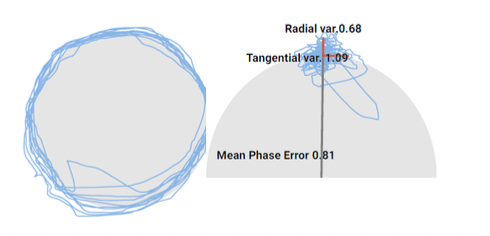 C. Eye tracking in relative left neck rotation 2 days after car accident.
C. Eye tracking in relative left neck rotation 2 days after car accident.
Treatment focused on cervical manual therapy to mitigate hypertonicity and tenderness. Concussive symptoms resolved 7 days after accident with focus on vestibular treatment, which is beyond the scope of this blog. Cervical re-assessment at this time showed improved smooth pursuit eye tracking parameters consistent with mild improved clinical signs and symptoms, although eye tracking parameters were still abnormal relative to neutral cervical spine position. After continued physical therapy management and manual therapy for a total of 2 weeks after injury, she was fully discharged with no clinical signs and symptoms and no smooth pursuit eye movement abnormalities across all cervical positions.
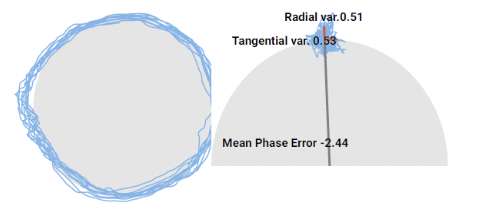 A. Eye tracking in neutral neck position at discharge.
A. Eye tracking in neutral neck position at discharge.
 B. Eye tracking in relative right neck rotation at discharge.
B. Eye tracking in relative right neck rotation at discharge.
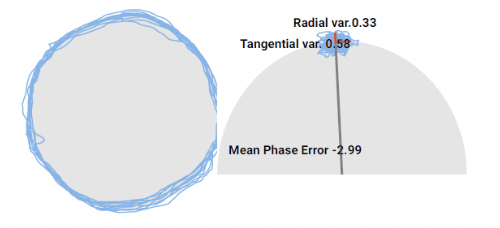 C. Eye tracking in relative left neck rotation at discharge.
C. Eye tracking in relative left neck rotation at discharge.
Of course, this is one case, and other patients may present differently; however, there is a definitive close association between improvements in smooth pursuit oculomotor measurements with subjective and objective clinical progression including neck pain, hypertonicity, and range of motion measurements. Clinical utilization of eye tracking in conjunction with physical examination can be imperative in the diagnosis of cervical contribution after acute whiplash as well as provide objective data to quickly guide the appropriate treatment approach. This early intervention can significantly decrease incidence of chronic neck pain and/or chronic whiplash associated disorders and the sequelae of further symptoms, which will allow us to achieve our ultimate goal to help patients make a full recovery and return to sport sooner.